Every emergency has two timelines.
The first is when the threat actually begins. The second is when people realize it’s happening.
Sometimes those moments are separated by minutes. Other times they’re separated by weeks or months. The larger the gap, the more complicated the response becomes.
Unlike a hurricane that appears on satellite imagery or a wildfire that announces itself with smoke on the horizon, infectious disease outbreaks often emerge gradually, quietly moving through communities before patterns become visible. By the time the alarm is raised, the challenge is determining how far it has traveled, who has been affected, and whether containment efforts can move faster than transmission.
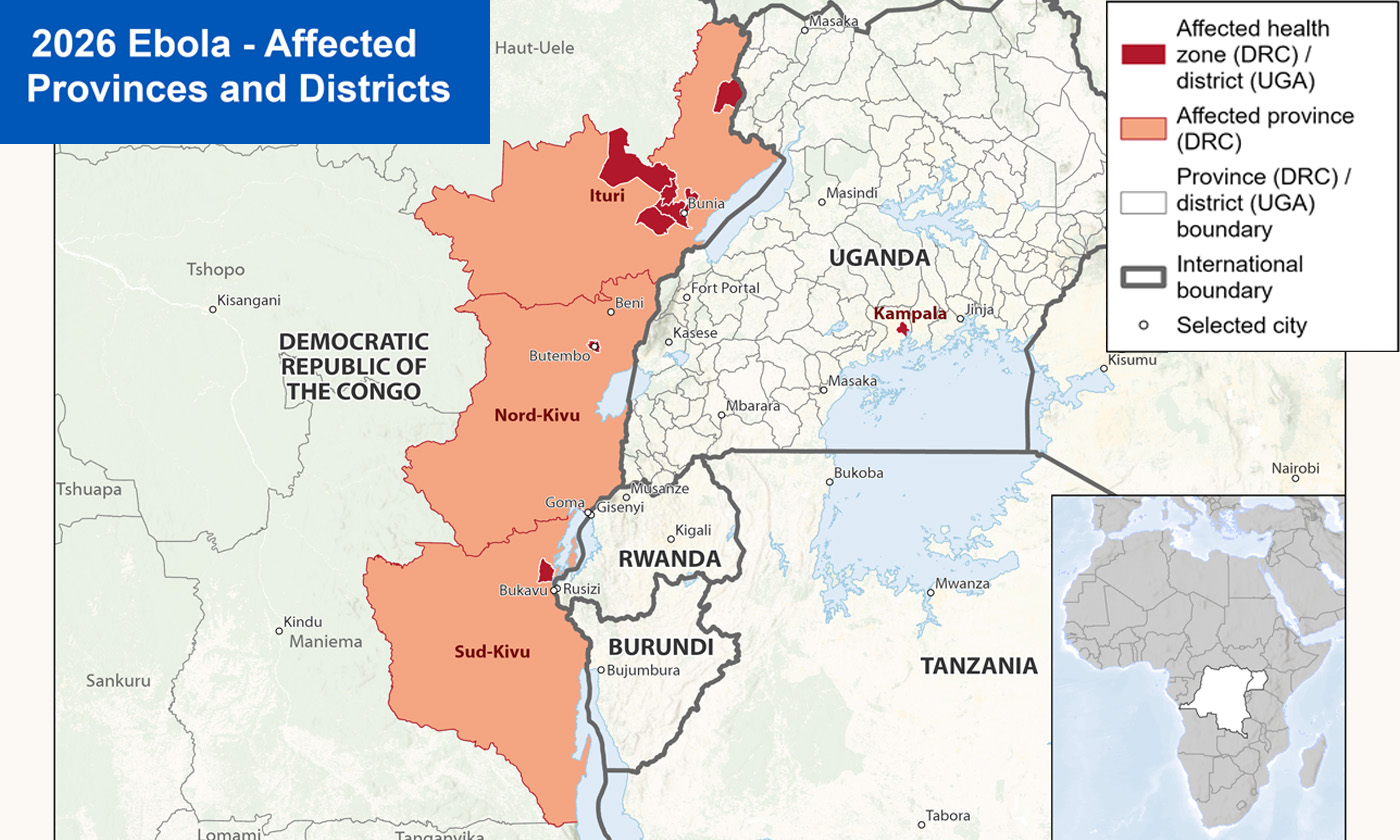
That uncertainty now sits at the center of the Ebola response in the Democratic Republic of the Congo (DRC) and neighboring Uganda.
The outbreak involves the Bundibugyo strain of Ebola, a relatively rare variant for which there is currently no approved vaccine or treatment. While researchers are evaluating experimental vaccines and therapeutics, public health officials must rely on more traditional containment measures: identifying cases, tracing contacts, isolating infected individuals, and monitoring communities for signs of spread.
Those efforts become exponentially more difficult when an outbreak isn’t discovered immediately.
According to the World Health Organization (WHO), evidence suggests the virus may have been circulating for months before it was formally identified.
“The outbreak had a big head start, and we’re still behind,” said WHO Director-General Dr. Tedros Adhanom Ghebreyesus while discussing the organization’s response efforts. That delay has created significant challenges for response teams attempting to reconstruct transmission chains and determine the true scope of the outbreak.
Unfortunately, containing Ebola (or the spread of any disease) is never solely a medical exercise.
The outbreak is unfolding in parts of eastern DRC where ongoing conflict, displacement, and security concerns complicate response efforts. Health workers have struggled to access certain communities and population movement across borders increases the difficulty of monitoring potential exposures.
Meanwhile, misinformation is undermining public trust.
Health organizations have warned that false claims circulating online are making it harder to encourage cooperation with contact tracing, testing, and treatment programs. During any outbreak, public confidence becomes a force multiplier... or a force reducer. Communities that trust health authorities are more likely to seek treatment, report symptoms, and follow public health guidance. Communities that don’t can inadvertently accelerate transmission.
The challenge is reflected in one of the outbreak’s most alarming statistics: WHO officials report that roughly 55% of known contacts are not currently being monitored due to insecurity, mobility, and access limitations.
Why you should care: For most organizations, Ebola itself is unlikely to pose a direct operational threat. The broader lesson, however, is highly relevant.
The current outbreak demonstrates how quickly risk can grow when detection lags behind reality. The virus began spreading long before health officials understood what they were dealing with. Once identified, responders were forced to manage not only the threat itself but also the consequences of lost time.
The same principle applies to virtually every organizational risk.
Whether it’s a cybersecurity incident, workplace safety concern, supply chain disruption, severe weather event, or emerging geopolitical threat, the gap between when a problem begins and when leaders become aware of it often determines the outcome.
Organizations can’t eliminate every risk. But they can shorten the distance between detection and response. The faster you identify a threat, the more options you have. The longer a risk remains hidden, the fewer choices remain available. |

